

Transcutaneous Pacing: Part 2
- Josh Kimbrell
- May 15, 2024
- 4 min read

TCP in the ROSC Patient: False Electrical Capture at 75mA
Josh Kimbrell, NRP
@joshkimbre
Judah Kreinbrook, EMT-P
@JMedic2JDoc
This is the second installment of a blog series showing how transcutaneous pacing (TCP) can be difficult and how you can improve your skills. We will be using redacted information from different cases where paramedics attempted TCP in the field. Details are edited and redacted to preserve patient anonymity.
In this call, paramedics arrived on scene to find a patient apneic and pulseless with CPR in progress by first responders (AED had an unknown unshockable rhythm). Per protocol, respirators, eye protection, and gowns were donned prior to contact. Patient had an unwitnessed cardiac arrest without bystander CPR performed. Paramedics continued compressions and ventilations (30:2 per protocol prior to advanced airway placement) and had an initial rhythm of asystole.
Crew obtained intravascular access and intubated the patient on the second attempt, confirmed with capnography. Epinephrine administered intravenously. After 13 minutes of ALS resuscitation, pulses were palpated indicating a return of spontaneous circulation. Initial vitals show hypertension (175/85), Atrial Fibrillation with RVR as seen in Figure 1, hypercapnia (99mmHg), and SPO2 of 100%.

Figure 1: Initial ECG shows Atrial Fibrillation with LBBB morphology and mild discordant STE not consistent with OMI.
After 5 minutes post-ROSC, the atrial fibrillation converted to a sinus rhythm. The crew transferred the patient to the ambulance and noticed weak radial pulses (BP unobtainable). They administered 10 mcg of push-dose epinephrine. Crew contacted on-line medical control to request sodium bicarbonate due to a concern for persistent hypercapnia (CO2 72mmHg) and were granted orders of 88mEq IV and ordered to expedite for transport.
Crew notifies the receiving ED of an incoming post-arrest patient and notes a sinus bradycardia on their monitor, as seen in Figure 2.

Figure 2: This rhythm shows a sinus bradycardia at a rate between 30 and 40bpm.
The crew immediately initiated TCP at a rate of 70bpm and slowly increased the current, as shown in Figure 3. Atropine and further doses of epinephrine were not administered.

Figure 3: TCP is started and the pacer spikes are followed by small phantom complexes and interspersed with native beats of the heart recognized by the demand pacemaker with a triangle and a pause in the pacer depolarization.
The paramedics initially set the current at 60mA. As seen in Figure 4, the current is higher, the phantom complexes are larger, but they do not have true electrical capture.

Figure 4: Pacer set to 60 mA with false electrical capture and native beats.
The crew increases this current to 75mA and documents an “improvement in patient status” with palpated pulses and a BP of 115/60. This set current is seen in Figure 5.
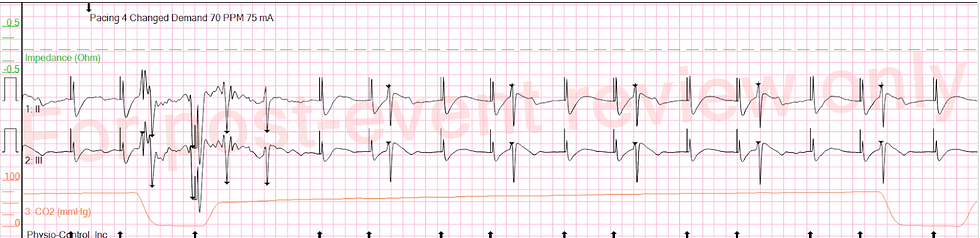
Figure 5: Current increased to 75mA with false electrical capture.
For the remaining 8-minute transport, TCP is continued with false electrical capture in Figure 6.

Figure 6: Here is false electrical capture with intermittent native beats.
On arrival at the ED, the leads are ripped off the patient and the pacemaker fires in non-demand mode for several minutes, as seen in Figure 7.

Figure 7: The false electrical capture with artifact gives way to ------- as soon as the leads are taken off the patient.
Pacing was continued in the ED, with identical settings. It’s unclear if the ED monitor showed false electrical capture, but if you had to bet on it… I’d suggest you bet on continued false electrical capture. Patient was transferred to comfort care and died in the ED.
Several learning points here.
First, this case shows how use of TCP in the post-ROSC period is common making adhering to a standardized ACLS algorithm difficult. While a 45-year-old patient with dizziness, diaphoresis, and confusion with junctional bradycardia and a BP of 72/46 has a relatively straightforward approach with administration of atropine prior to TCP initiation (as long as intravascular access is already or can quickly be obtained). In contrast the post-ROSC patient with a sudden drop in heart rate may be peri-arrest and with pads positioned already, TCP may be a reasonable choice. Paramedics must recognize, however, that re-arrest is a dangerous and lethal condition that is more difficult to recognize with false electrical capture showing an arcing artifact that the crews interpret as a QRS complex.
Second, this case demonstrates that the presence of a monitor visualizing a native complex, in this case the LifePak 15, flagged providers with the characteristic “triangle” akin to synchronized cardioversion, should result in a pause. If the crew had taken the time to analyze the ECG (admittedly difficult in the prehospital environment with numerous other obstacles to manage), they would have noticed that the demand pacer was recognizing an underlying rhythm close to 60bpm, which may indicate that TCP is not required.
Lastly, this shows how phantom complexes in false electrical capture can be difficult. With the native beats quickly following the pacer spike, the paramedics rightly reported they palpated a pulse. They see this phantom complex along with an increase in blood pressure (perhaps from the push-dose epinephrine, or the sodium bicarbonate, or as part of an early hemodynamic recovery post-arrest) and think their intervention is successful. Approach TCP with skepticism. Success in this procedure is rare and interpretation is difficult. As we will show in future posts skepticism is critical to learning to improve your skills.




Comments